


Antibodies, T-Cells, Omicron, and Endemic Covid
Predictions and Literature Review

With Omicron kicking off what is likely to be the largest wave of the pandemic, the question I want to answer is what to expect from our current vaccines in terms of ongoing protection, both antibody and T-cell protection, and if that can get us to an endemic state.


Here are my predictions after evaluating the evidence, which is all summarized in this post.
Antibody protection from all vaccines and boosters will decrease over 6 months from last vaccine, to the point of no longer preventing infection given an exposure [85%].
Long run protection against severe disease will continue against current variants, despite protection against infection declining [90%].
Long run ‘steady state’ endemic covid, which we can define as having a seasonal pattern similar to the influenza, will require the full population to have a robust T-cell response to the virus, which cannot be gained from vaccination alone, given our current class of vaccines. [70%]
Adenovirus vaccines provide a stronger T-cell response, and less decline in antibodies over time compared to mRNA vaccines. This is what the data shows so far, and I predict it holds up even as we create additional boosters, and gather more data. [65%]
We should be boosting, or supplementing, with J&J (or another adenovirus vaccine if you received a mRNA initial course. This would lower immediate benefit, but would have better long-run properties, defined as lower severity to infection compared to an mRNA cohort. [50%]
Boosting won’t stop infection from Omicron, but the T-cell response, combined with the refreshed antibody count will lessen the severity compared to no booster. [95%]
Lockdowns and isolation in Western countries cannot meaningfully contain Omicron, due to its level of infectiousness and antibody escape [98%].
The more intense Chinese lockdowns and isolation cannot meaningfully contain Omicron, due to its level of infectiousness and antibody escape [75%].
When reading the research, I looked to triangulate the evidence from two directions:
Scientific mechanisms (e.g. neutralization assays).
Empirical studies on outcomes in the population.
Antibodies from vaccines wane quickly, and are not robust to new variants, suggesting re/infection is an inevitability.
We are observing that antibodies wane, which reduces protection against infection. While boosting clearly helps prevent infections against Beta or Delta, it seems unlikely it will protect against infection by Omicron. However, Pfizer is saying that the boosted vaccinated have 70% protection against severe illness (compared to 93% against delta). The evidence for this seems pretty straightforward: Antibodies don’t do nearly as much to neutralize Omicron (sure would be cool if we could boost Omicron, rather than the wild-type strain…).
Class of evidence: Scientific Mechanism.
Title: Third BNT162b2 vaccination neutralization of SARS-CoV-2 Omicron infection
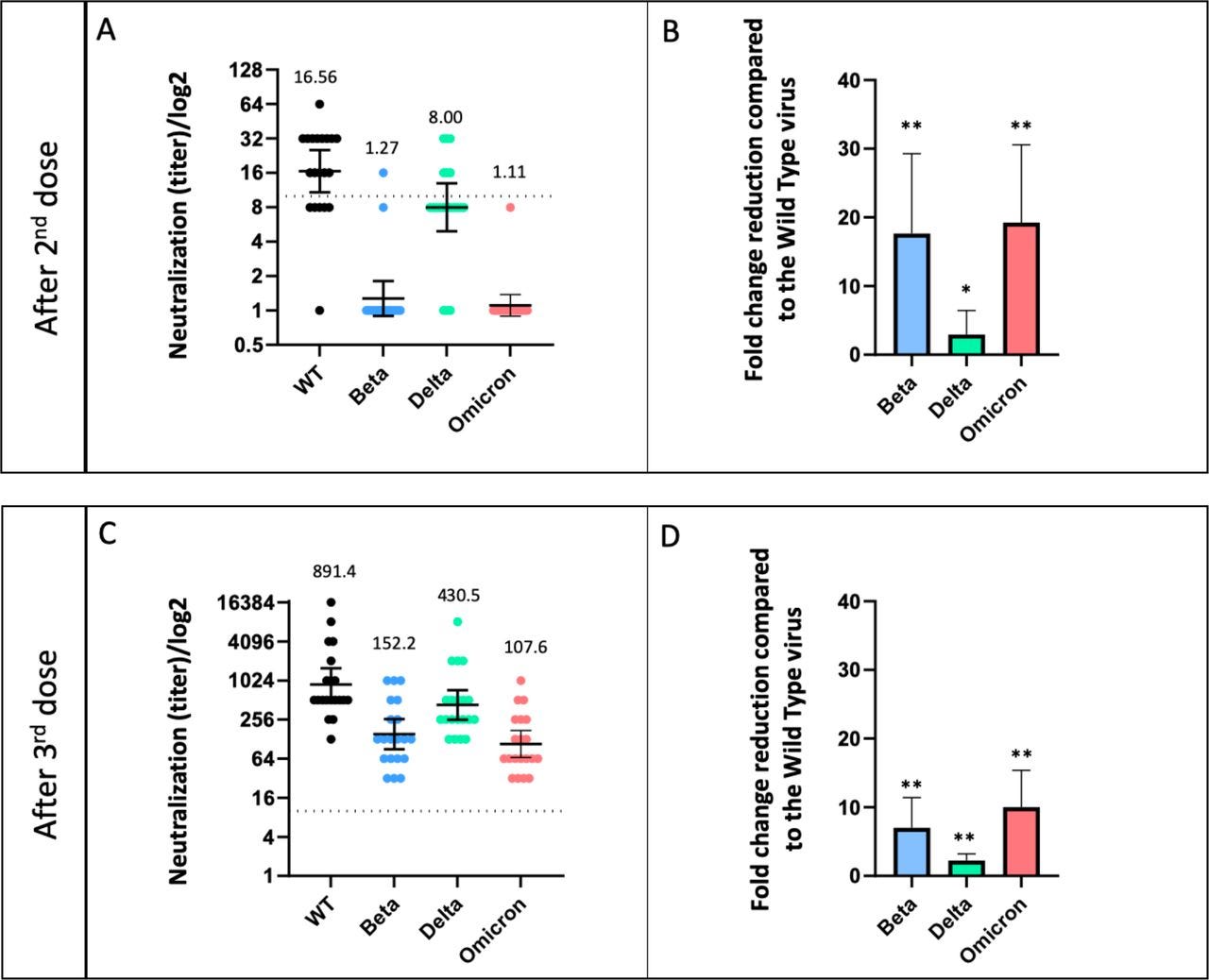
This paper is a preprint that came out December 14th, 2021, and effectively finds that neutralization against Beta and Delta decreases more than 5 months following the second BNT162b2 (Pfizer) dose, and offers no neutralization against Omicron. Neutralization is restored after a booster, but they note the durability of the third dose is yet to be determined (since we have very little historical data here).
This paper is a preprint that came out December 13th, 2021. Similarly, this paper finds that neutralization decreases, and they speculate it’s high enough that breakthrough infection or reinfection could continue to happen to Omicron, even with a booster.

Title: mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant
This paper is a preprint that came out December 14th, 2021. Same deal, with the key figure and commentary from Eric Topol below.


Class of evidence: Empirical outcomes.
This paper was published in The Lancet October 4th, 2021 (pre-Omicron). This paper finds that immunity wanes with time. This is corroborated by the declining antibodies measured above.

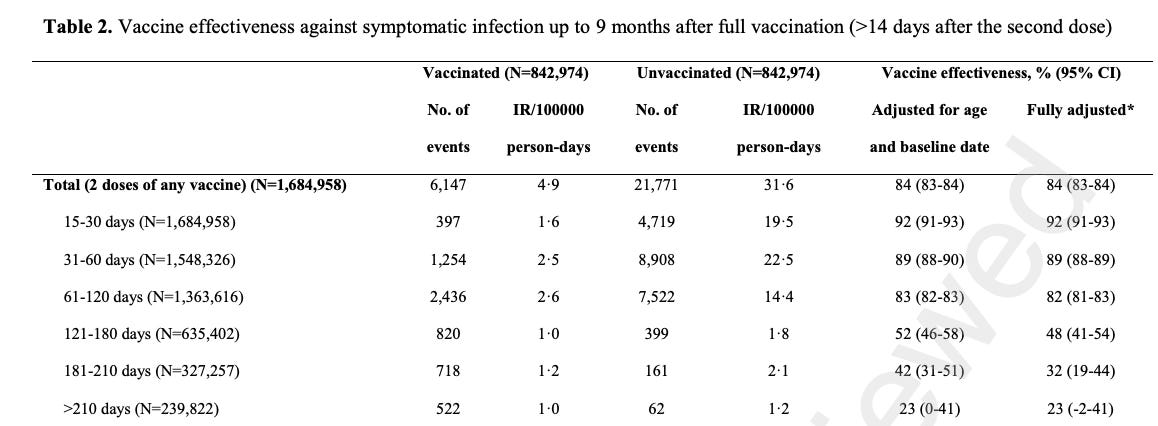
This paper was published in The Lancet on October 25th, 2021 (pre-Omicron). The methodology constructs longitudinal treatment and control groups (vaccinated and unvaccinated). They attempt to approximate a randomized control trial by matching on age and sex, despite there being clear differences in severe comorbidities varying between the two groups.
The omitted variable bias is probably less of a confounder in younger populations, which have a low base-rate of comorbidities, although older populations will be biased. And unfortunately their choice of age cut-offs is ridiculous, with some tables breaking ages into two groups, greater than 80, and less than 80 (the less than 80 group will still be dominated by deaths of people 75 to 80).
And yet I can’t find anything better. So let’s see what we can recover from this.
The key take-away is that we have outcome oriented data that does confirm that declining antibodies represents a material decrease in preventing infection as time from vaccination date increases. It’s much more difficult to make any inference from this paper on death, as the power to detect is is too low in younger populations, and omitted variable bias is too large in older populations.
[Note: In the later time-periods it is actually higher than the unvaccinated. There are a small handful of biases that could cause this, and IMO we shouldn’t read too far into it].
Summary:
There are practical consequences of waning antibodies: The first is avoiding infection indefinitely is likely not possible. Even if you continue to receive boosters, variant escape will decrease the likelihood they stave off infection, as they already have. And as new variants come about, the lag between their existence and an updated vaccine is likely too long to avoid an infection without ongoing lockdowns (this perhaps didn’t have to be the case).
Until then, we may continue boosting, and getting infected anyway. To some this is fine, to others it’s dystopian and signals a never-ending bio-state (admittedly this has become more of an issue that I originally predicted). I think it’s maybe a moot point anyway, since a pan-coronavirus vaccine (if it ends up passing trials) would be better than constant boosting.


Regardless, I want to know that even if many in the population don’t get a recurring booster, or if my parents get infected right before their next booster, or if I got Omicron last night when I went out to dinner, what should I expect? For this we need to consider T-Cell immunity.
Enduring T-Cell immunity.
Antibodies can bind and prevent infection. T-Cells cannot prevent infection, but can prevent an infection from having a severe outcome. Killer (CD8+) T-Cells seek out and destroy viruses. Helper (CD4+) T-Cells stimulate antibody protection, and can create killer T-Cells. Given that we see antibody rates waning, T-Cell immunity is particularly interesting.
I don’t want to stress about whether my antibodies are waning, or how susceptible I am to infection, or whether some new variant will render my antibodies useless. This is similar to other other circulating respiratory viruses we live with, which would kill a naive population (e.g. an indigenous tribe), but which I really don’t care about, even though I get (re)infected constantly.
I want to have that same confidence for covid that I have a ‘lower-level’ robust persistent immunity. Is this a reasonable expectation? And if so, how do the vaccines support this? The short answer seems to be that vaccines do give T-cell immunity, but that the mRNA may offer less protection than adenoviruses. We also know that vaccines only offer T-cells for spike epitopes (an epitope is the part of an antigen molecule to which an antibody attaches itself), and this may be why natural immunity is more robust.
Title: “SARS-CoV-2 human T cell epitopes: Adaptive immune response against COVID-19”
This paper came out in July 2021 in Cell Host & Microbe, and provides a review of the literature, and summarizes the current understanding of T-cell immunity. A few key excerpts from the paper are below:
While it is not expected that preexisting T cell reactivity might protect against infection, it is possible that preexisting SARS-CoV-2 cross-reactive T cells might modulate disease severity, as reported by a recent study (Sagar et al., 2021), or might even modulate vaccine responsiveness, allowing for a faster or more vigorous response.
Because of the high number of different epitopes reported, as noted above, and because of the large breadth of epitopes recognized in any given individual (estimated to be an average of 19 class II and 17 class I epitopes per person, genome-wide, and 9 if only the spike protein is considered), as suggested by one study (Tarke et al., 2021a), it appears unlikely that the new variants will escape T cell recognition at either the population or individual level.
In light of the data that indicate that T cell escape is not occurring (Tarke et al., 2021b), it is also relevant to consider the immunological and virological features that make T cell escape by SARS-CoV-2 unlikely. First, as noted, the broader the T cell response, in terms of epitopes, the less likely viral escape becomes, because any individual epitope that can escape through viral mutation would represent a small fraction of the overall immunity and thus represent a small selective pressure. Given that SARS-CoV-2 is a large RNA virus, the breadth of the CD4 and CD8 T cell responses is not surprising, per se.
so tl;dr, they expect that T-cells modulate severity, and the virus is less likely to escape T-cell immunity, but also we see that the spike protein (what most vaccines are built around) is only a subset of all epitopes.
This paper was written prior to Omicron, but the prediction they made that-T-cell escape is not likely to happen, seems to have been vindicated. as most of the CD4 and CD8 epitopes are preserved between Omicron and legacy covid.


In addition, epitope conservation on only the spike protein is high as well, which is how our vaccines are constructed.

Class of evidence: Scientific Mechanism.
Title: "Rapid and stable mobilization of CD8+ T cells by SARS-CoV-2 mRNA vaccine"
This paper came out in July, 2021 in Nature, and found that the mRNA vaccine does generate T-cell immunity.
This paper goes pretty deep into the nerdy details (reading this paper was a stretch for my scientific ability, and I had to wiki a lot of terms) and their analysis compared mRNA vaccination with natural infection. They found that the CD8+ T cells are similar, but they note: “Compared with natural infection, however, the early memory pool of spike-specific CD8+ T cells after vaccination exhibits a different memory T cell subset distribution that may affect long-term maintenance characteristics.” Basically the take-away is the distribution of T cells is different between vaccination and natural immunity. Is this bad? good? Unclear.
However, they do provide evidence that T-cells do not wane. In the figure below you can see that the CD8+ T-Cells remain elevated following vaccination, and don’t decline to the same extent of antibodies.

Title: Differential Kinetics of Immune Responses Elicited by Covid-19 Vaccines
h/t


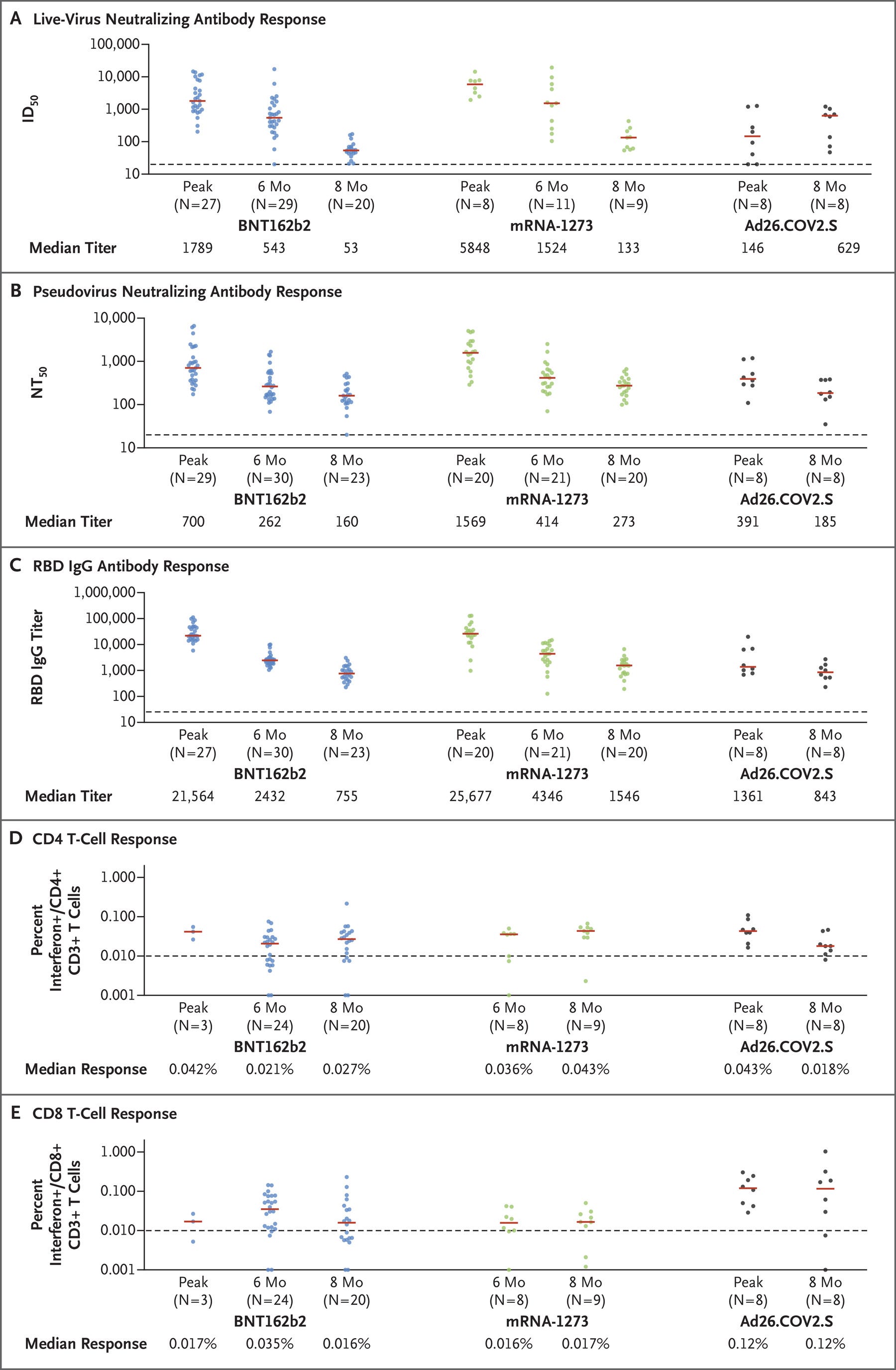
This paper came out November 18th, 2021, and is in the New England Journal of Medicine. They start by similarly finding that neutralizing antibodies decline sharply over 6 months, and then evaluate T-cell responses.
What’s very interesting here, is the adenovirus antibodies don’t seem to wane: “The Ad26.COV2.S [Johnson & Johnson] vaccine induced lower initial antibody responses, but these responses were relatively stable over the 8-month follow-up period, with minimal-to-no evidence of decline.” If this is true, why aren’t we boosting mRNA with J&J? This seems like a big deal, right? I initially thought perhaps the J&J recipients were younger, but they appear to be older [Supplementary appendix].

In the below plot, we see pfizer, moderna, and J&J at peak and 8 months. As the story goes, moderna holds up better than pfizer, but they both are on a clear downward trajectory. J&J has a much weaker initial antibody response, but it seems to hold up better.
Keep in mind, what we’re doing is a glorified trend-line forecast drawn through a couple points — still, it’s all we have to go off of. The dispersion between groups is also pretty high, and the sample size for each group is roughly 25. So there are mRNA recipients who will have a better long-run response than J&J, even though the means show J&J holds up better on average. Maybe we’re just being fooled by randomness? Although my personal gut prediction is that this is a real enough signal that I predicted it’s 70% true.

Their findings for T-cells were that “At 8 months, the median CD8+ T-cell responses were 0.016% with the BNT162b2 [pfizer] vaccine, 0.017% with the mRNA-1273 vaccine, and 0.12% with the Ad26.COV2.S vaccine. With all three vaccines, T-cell responses showed broad cross-reactivity against SARS-CoV-2 variants”
One thing you can notice is that the T-cell response is lower in the mRNA vaccines than the adenovirus vaccine by an order of magnitude. Again, we have to be careful to not assume a linear relationship between response and efficacy, although it seems reasonable to predict that a higher T-cell response reflects better immunity, I suppose there is no rule that says T-cell response is highly nonlinear. Perhaps this is something a virologist would have great intuition on, that is a mystery to me.
Ultimately, It’s hard not to read this paper and come away from it thinking J&J (and perhaps other adenovirus vaccines? Novavax? AstraZenica?) are underrated. It seems as though everyone gets really excited about antibody responses within the first three weeks, whether from the original vaccine, or the booster, but are people paying attention to the full time-series?
Part of this may also be related to the idea that all infections are bad and need to be avoided, in part due to the risk of long covid. While I get that, clearly our vaccines don’t protect against infection to Omicron. As a result, what is more important for civilization is that we are protected from severe disease, and natural infection provides particularly robust immunity. This is what lets us get to endemic steady-state.
Class of evidence: Empirical outcomes.
Observational studies are far more recent, as the more interesting data has only been generated in the last two months. This is due to the fact that the questions we have about T-cell immunity, are how do they protect against new variants, and how do they work when antibodies wane, both pieces of data that weren’t generated for the first ~6 months of vaccination data.
This is a pre-print, and has already been summarized pretty well, so I’ll reference the tweet-thread by Andrew Lilley below.




This is comparing ChAdOx1 (AZ) to BNT162b2 (pfizer). However, the AZ vaccine is behaving how we would expect J&J to behave based on the evidence of higher T-cell concentrations are higher in the long-run, but initial antibodies lower. I’m guessing this isn’t a coincidence, as they are both adenovirus vaccines, and I’m going to count this as evidence that adenoviruses are more robust.
Title: Some Danish Powerpoint.
Again, we see similar data to above, with further emphasis on natural immunity (the slide is in Danish, but the tweet explains what the lines are).


Summary:
The practical conclusion of this is that natural immunity seems the most robust, and that adenoviruses maintain higher T-cell and antibody concentrations over time. It’s more difficult to find methodologically robust observational (or randomized) studies that measure this and correlate it to outcomes. In part due to the fact that this is happening right now, and in part due to a failure of governmental data gathering.
Upon reviewing the evidence, I’m also finding myself less interested in what prevents infection, primarily because it seems all of our vaccines are too leaky to prevent infections given Omicron, and given that Omicron is insanely infectious, it’s basically too late to invent leak-proof vaccines. To be honest, I think most of us are going to get Omicron. Extreme isolation and lockdowns may postpone it, but I think it’s just too infectious. I also don’t see any end game, even if we do postpone it, other than natural immunity.
It also seems the cost of avoiding infection for the vaccinated and relatively younger population, no longer outweighs the benefits. Considering that…
Antibodies wane over time for most vaccines (or are never high to begin with), and we seem to be in a position where even if they didn’t, variants will break past the antibody defense layer. (speculation: it may even be better to get a breakthrough infection while our antibodies remain high).
Our spike based T-cell immunity from vaccination hopefully protects against severe infection, but a natural infection will give us T-cell responses to all epitopes.
The joint vaccinated and then infected state provides what appears to be super immunity, which is significantly more protective. We also have good reason to believe the robust T-cell response generated in this state will allow us to return to a far more normal life.
What’s the alternative? Ongoing isolation, lockdowns, and despite that we will still probably get infected anyway.
I think things are going to get a little weird, as we are in the middle of the biggest wave to date, and a lot more people are going to die. But if this is true, the combination of vaccinated and natural immunity that sweeps over our population will end the novelty of covid, and usher in a new endemic era.
Injected-vaccine-induced T cells home to the skin where they are useless. Respiratory infection induced T cells home to the lungs, nasopharynx where they protect.
Most T cell researchers make the mistake of ignoring this basic fact and come to erroneous conclusions.
Mechanisms of T cell organotropism
https://pubmed.ncbi.nlm.nih.gov/27038487/
"Differential Kinetics of Immune Responses Elicited by Covid-19 Vaccines"
I too had the question of how T-cell data they recorded translates to severe disease outcomes. On paper a 7-8 times drop in the mRNA vaccines vs the adenovirus vaccines seems relevant but I have no clue what the real world meaning of that it is. The authors do comment, "With all three vaccines, T-cell responses showed broad cross-reactivity against SARS-CoV-2 variants (Fig. S6)." but this is as far as they elaborate..